The six basic principles of wound management for low-resource settings
1 Jul 2024
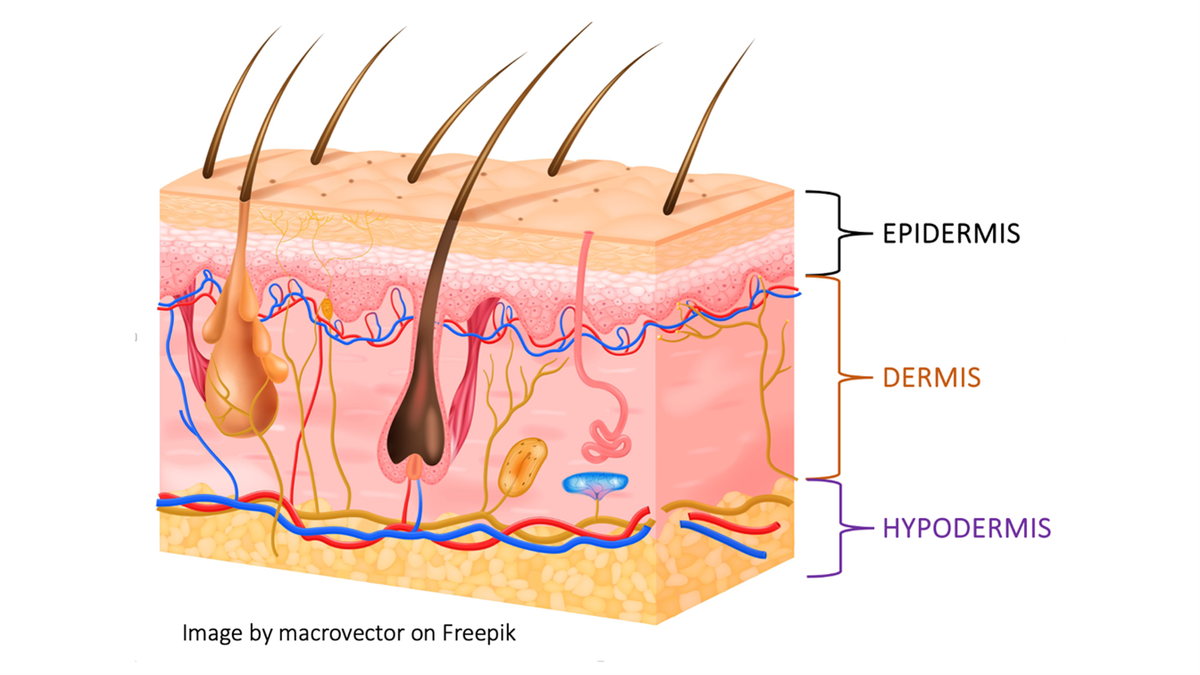
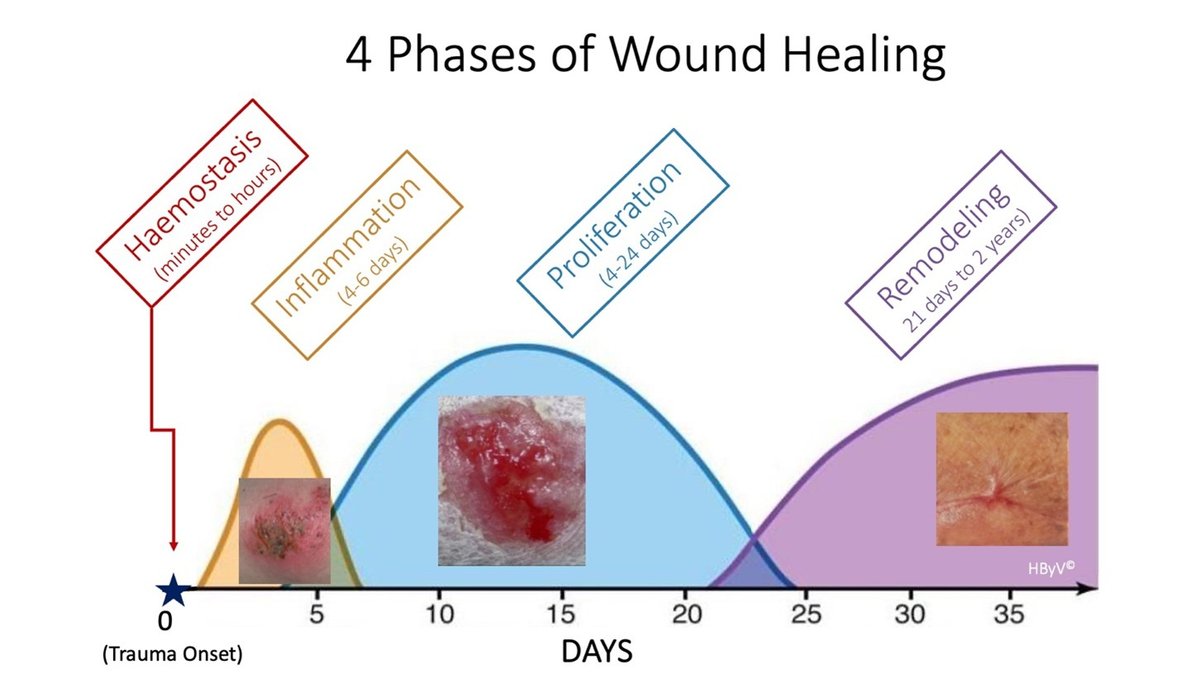
Basic skin anatomy and wound healing physiology
Many health caregivers are not familiar with the key principles surrounding the selection of wound dressings that are required for successful healing. Effective dressings are selected to recreate the body’s normal conditions, so understanding the basic anatomy of the skin and the wound healing processes is essential to inform the appropriate choices.
3) Protect wound and peri-wound skin from further trauma
Since wounds are fragile, one must prevent additional damage that may occur to the wound bed or the weakened skin.8 Mechanical damage occurs frequently when dressings stick to the wound and/or adhesive bandages are harshly removed from the skin. Chemical damage can occur when excessive disinfection is used, as many such products, especially if used for too long, can be harmful to the wound bed. Lastly, excessive dryness and coolness can lessen cells’ activity and impair healing. Thus, we recommend using nonstick dressings and soaking them, and adhesives, with saline or potable water before removal (Fig. 5). Use of saline or potable water to clean wounds is preferable; only use disinfectants on locally infected wounds.


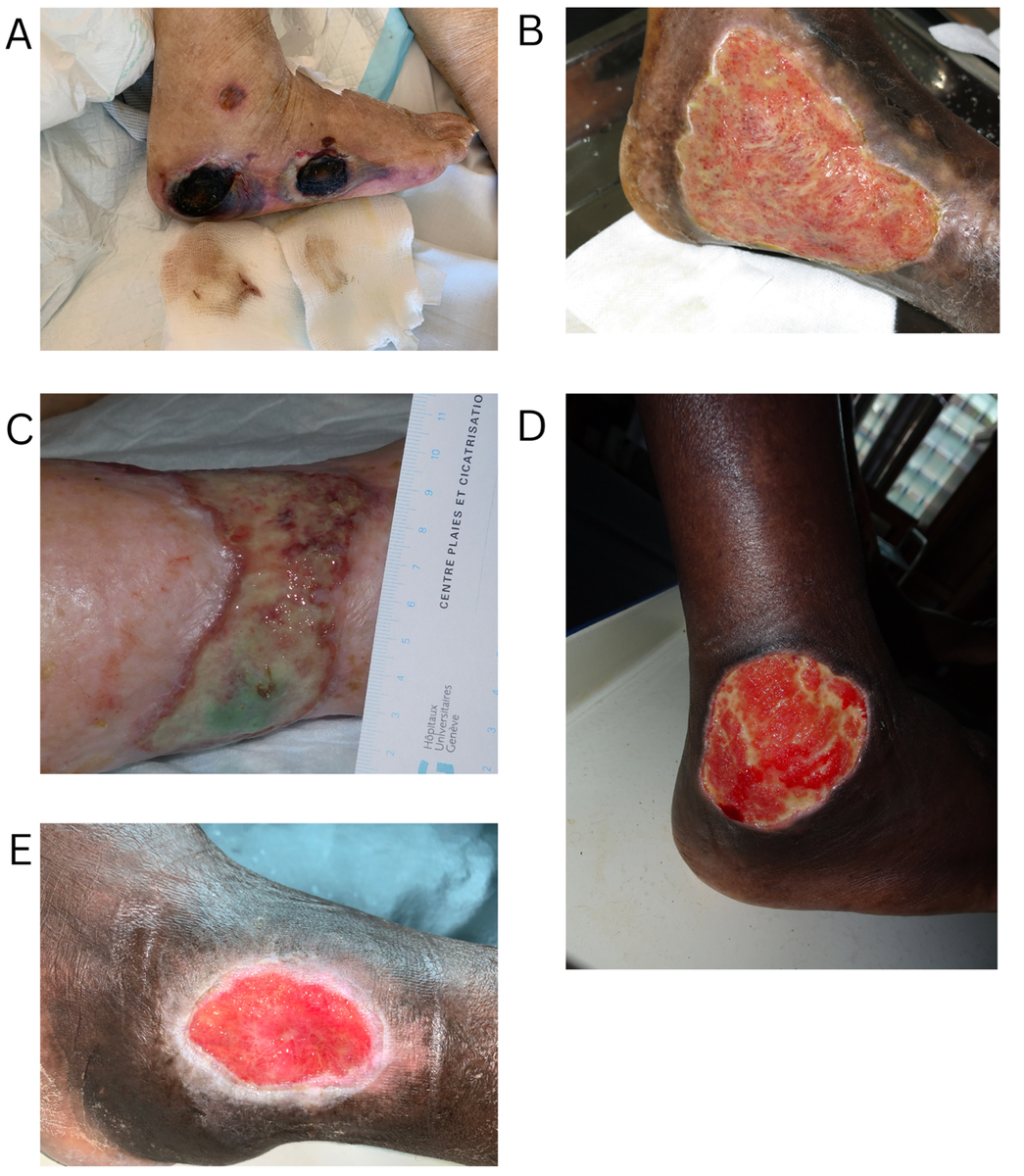
6) Promote a clean wound bed and control infection
The wound bed is the foundation for good wound healing; it must be clean and free from infection.8 First, all necrosis and fibrin must be removed through a process known as debridement. Large wounds will need instrumental debridement to remove dead tissues (with scalpel blade, scissors, curette). After removal, the fresh wound bed should be rinsed and cleaned with potable water or saline to clear out excess microbes or debris (Fig. 6).


We encourage the reader to learn more about wound care at OpenWHO (see Wound management in resource-limited settings, In Press).